Chicago’s Ujimaa Medics bring a racial justice and cultural specificity lens to community health care through mutual aid.
“The western medical-industrial complex has often left out or been directly harmful to Black people.”
In this feature, we ask organizers involved in mutual aid projects to share a little bit about their work. We understand mutual aid work as the part of social movement organizing that meets people's direct needs. Unlike charity work, however, mutual aid is part of a broader strategy to address the root causes of injustice by mobilizing people to dismantle structures of domination and build the world we want.
Mutual aid efforts are proliferating as people respond to the Coronavirus pandemic. You can track emerging projects at mutualaidhub.org, and we recommend checking out this useful guide from Mutual Aid Disaster Relief about how to start COVID-19 mutual aid projects and do the work safely and effectively. We also recommend the Big Door Brigade’s Mutual Aid Toolbox and this short mutual aid explainer video, for starting conversations about what mutual aid is and why it is a vital tactic to expand right now.
This week, we had the honor of interviewing Ujimaa Medics.
“Mutual aid is part of a broader strategy to address the root causes of injustice.”
Dean Spade and Roberto Sirvent: Can you please tell readers of the Black Agenda Report a little about your background and the mutual aid work you have been involved in?
Ujimaa Medics: The Ujimaa Medics (UMedics) co-founders are Martine Caverl and Amika Tendaji. UMedics is a volunteer-based Black health collective that was developed in response to health disparities and the problems that follow widespread historical and immediate trauma in Chicago's Black community. Martine and Amika became friends about 15 years ago. Amika grew up watching her grandmother, a home health nurse, nurse her patients, but also teach her patients’ families how to administer care in her absence. Martine became interested in health and preparedness after visiting New Orleans to provide re-building support to grassroots organizations after Hurricane Katrina. We are trained as street medics and have served at marches, land occupations, sit-ins, and a hunger strike. Both of us have completed Community Emergency Response Team training (CERT), and are also involved with the Black Survival Network, which has been teaching outdoor leadership and emergency survival skills to Black folk for over 40 years. We both were in a collective that sent a delegation from Chicago to Haiti, which transformed into a new formation that focused on teach-ins, raising funds to send directly to Haitian-led, grassroots organization, and protesting the waste of the American Red Cross after the 2010 Earthquake.
“We are trained as street medics and have served at marches, land occupations, sit-ins, and a hunger strike.”
During our Haiti solidarity work, we lost a young person who was shot blocks from the University of Chicago and passed away en route to a hospital far on the other side of town. We supported the resulting victorious campaign to re-open a trauma center and also believed that our people needed immediate skills to help until a higher level of care could arrive. The pilot workshop took place in Martine's living room in 2014, starting with close friends and family. A year later in 2015, we held our first Train the Trainer to officially launch our collective. We have reached almost 2,000 people through our workshops mainly on basic and advanced gunshot first aid, in addition to asthma, seizure, and diabetes community care. We’ve been from Chicago to Detroit, Cleveland, Milwaukee, New Orleans, Washington DC, and Seattle. We have done this with no staff, just a small collective of dedicated volunteers. A few people credit members and workshop participants with saving their lives.
How does this work fit into the broader struggle for change you are working on? How does it mobilize for change rather than merely being a "band-aid" on a harmful system?
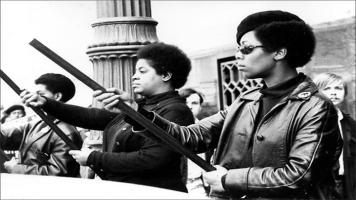
Trying not to apply a band-aid over a bullet wound is a great challenge for mutual aid groups. Often the people with skill sets needed for mutual aid acquired them in harmful institutions, or institutions that promote a savior ideology. As we said above, we take our name from a Kiswahili term (Ujima) for “collective work and responsibility.” While our members and supporters who are nurses, physicians, and emergency medical personnel are quite a credit to their profession and are very important to the work of our organization, the western medical-industrial complex has often left out or been directly harmful to Black people. We see ourselves carrying on a tradition that calls down plant medicine healers, granny midwives, The Black Cross Nurses Association, the Black Panther Party’s medical programs, movement medics, and health justice organizers who’ve shown us today that we must feel responsible to provide care and teach caring for ourselves and the folks in our communities. We ground ourselves in the reality that freedom for Black People includes the well being of our own bodies and those of our community.
Have you seen dangers of co-optation of the mutual aid work you have done? What structures or methods have the organizations or projects you work with put in place to address that danger?
While there are local groups that have been teaching community GSW trainings and have been able to acquire far more funding, some of those efforts appear to lack the racial justice lens and cultural specificity of what we do. We’re deeply grateful that we haven’t yet faced the kind of co-opting other mutual aid groups have. The medical-industrial complex and capitalism depend on us being willing to turn over all autonomy over our bodies to their profit model. We employ largely the same strategy that all freedom fighters have employed, that we are stronger together. We keep ourselves deeply rooted in a very left, organizing community with a clear focus on racial political analysis. We look to the past to remember many others have done what we’re doing now in far more oppressive circumstances, many still are in the global community. We try to love and support each other as if our very lives depend on it, because we recognize it very well might.
What are the pitfalls of mutual aid work, from your experience?
As we mentioned earlier, folks with skills associated with aid often come from the military, institutional medicine, or a position of material wealth and social privilege. They might see themselves as providing aid, a service, or saving people. Often groups aren’t developing relationships with organizations and leaders from that community. Mutual aid groups sometimes lack the cultural and logistical context that organizers can provide, and do not always work closely with existing grassroots infrastructure. Black folk attempting to build mutual aid projects are often very burdened with financial and capacity realities, and mutual aid groups don’t always interrogate racial dynamics enough to create space to listen to what Black leaders are saying their people actually need. We prefer the collective work and responsibility framework: we aren’t trying to be heroes, we believe our liberation is bound collectively and we are thusly responsible to the greater collective. Medical and disaster response knowledge is often informed by a savior model that has proven faulty time and again. We believe everyone can learn skills to heal and be healed and our greatest strength is in the many working together, not a few propped up elite. When we share skills or provide services under the banner of mutual aid, it’s not charity, because we are very clear that it’s an exchange between people that are working toward justice and helping each other get there. We also know that some of the kinds of skills and tools shared by first aid groups (ours included!) were gleaned from and developed in wars. We believe that this is knowledge that should be distributed to everyone, and mainly to the people who have lost the most in war. So it’s important to teach this knowledge with respect for the lives lost and suffering that it took to develop it, and to use it in service of liberation.
Do you think mutual aid work has any special or particular role in the current conditions/crises?
As disasters from the climate crisis and war rage on its incredibly important for us to recognize that the best help we can get is probably from each other, we are the best hope we have, and we are the most invested in reaching our most directly impacted and marginalized. Katrina and indeed our whole history as African people on this land has certainly taught us that no one will love and protect us like we will, so we have to spread and sharpen our survival skills while working for climate justice, against war, imperialism, racism, homophobia, transphobia, misogyny, capitalism, and the harms of the medical-industrial complex. We have to learn from and uplift the struggles of our global family while honoring the wisdom and lessons of our ancestors. We have to reject white and U.S. savior complexes and see those experiencing illness, poverty, war, detention, collapsed government, those crossing borders as ourselves and promote an urgency around protection and healing.
Do you have ideas about how mutual could expand or mobilize more people?
UMedics sees itself as a base-building organization, although the way we go about it is different from groups that are focused on direct action or digital organizing. We are taught to give overall autonomy of our bodies to a profit-based medical system and that’s hard to shake. It’s hard for our folks to think someone in mortal peril could be helped by me, and I can learn skills well enough to teach others. The more that we promote agency and mutual capacity over disaster voyeurism, the more we build up grassroots infrastructure and lessen dependency on large NGOs, the more we expand, the more we learn from our neighbors and understand when the chips are down we are all we’ve got, the more we expand and mobilize. We need to create delicious invitations to learning skills or at least practice community care consistently by offering to teach what we know as often as we can. We also practice small ways of skill-building and collective work by often suggesting things like if you can swim find a friend willing to learn from you, ask folks if they have their inhaler, ask folks how their bodies are doing, how the bodies of their loved ones are doing and let them know what you are able to offer, ask people if they need reminders for their medication or help to create an emergency plan.
Are there any examples of other mutual aid work, historical or contemporary, that particularly inspire you or that you have used as a model?
As an all-Black collective, we receive inspiration from maroons, palenques, and quilombos. We’re here because of granny midwives. Root workers. Church mothers who served elders, the ill, and new parents in their communities. The health programs run by the Panthers and SNCC. Underground midwives and abortion providers. Those who picked up skills in the military and brought those back to their people. Perhaps this doesn’t completely qualify as mutual aid, but there is also inspiration from some regional medical programs that have grown out of rebellions such as the Zapatista and Garifuna health networks. We are also inspired by the solidarity for global health growing out from Cuba. Our enslaved ancestors who made healing magic from very little were the picture of mutual aid. But more immediately, we love the work of People’s Community Medics and the Anti-Police Terror Project in Oakland, Feed the People and the Kola Nut Collaborative in Chicago, bail relief organizers, the Icarus Project, the Free Black Women’s Library, the Detroit Community Black Food Security Network, everyone who mobilized to provide water resources to the people of Flint, the whole international street medic community. Those are just the ones that come to mind. We can’t name everyone, but we know there are countless efforts going on where we have kindreds sharing skills, resources and tools with their people. We don’t know who you all are, but we thank you.
What can readers of the Black Agenda Report do to support your work?
We love monetary and supply donations. We love people talking about our work and those of other collectives like ours. We value stories that can help inform our work. We also are supported by all people struggling for liberation, against capitalism, war, imperialism, homophobia, misogyny, racism, transphobia, and those who fight for our planet and our water. We also value research on the history of those whose shoulders we stand on, and sharing their stories. If you are working to build up your community for resilience, strength, and unity, you already support our work.
Dean Spade is the creator of the mutual aid toolkit at bigdoorbrigade.com. He has been working in various poverty-focused and abolitionist mutual aid projects for the past 20 years. He is the author of Normal Life: Administrative Violence, Critical Trans Politics and the Limits of Law (Duke University Press 2015). His video projects and writing are available at deanspade.net.
Roberto Sirvent is Professor of Political and Social Ethics at Hope International University in Fullerton, CA, and an Affiliate Scholar at Yale University’s Interdisciplinary Center for Bioethics, where he directs the Race, Bioethics, and Public Health Project. He is co-author, with fellow BAR contributor Danny Haiphong, of the book, American Exceptionalism and American Innocence: A People’s History of Fake News—From the Revolutionary War to the War on Terror.
COMMENTS?
Please join the conversation on Black Agenda Report's Facebook page at http://facebook.com/blackagendareport
Or, you can comment by emailing us at comments@blackagendareport.com


 “It is perfectly clear that the war of aggression waged by Morocco against the [Western] Saharan people is a purely colonial war.”
“It is perfectly clear that the war of aggression waged by Morocco against the [Western] Saharan people is a purely colonial war.” The Congressional Black Caucus electoral strategy has turned the 2026 midterm elections into a dumpster dive for corporate interests and Zionist approval.
The Congressional Black Caucus electoral strategy has turned the 2026 midterm elections into a dumpster dive for corporate interests and Zionist approval. The Democratic Party's continued support for Israel's genocide is not just a moral and political liability but also an economic one which impacts its voters, yet the party refuses to frame it as such.
The Democratic Party's continued support for Israel's genocide is not just a moral and political liability but also an economic one which impacts its voters, yet the party refuses to frame it as such. "hand ‘em another $350 billion to fight Communism?" is the latest from BAR's Poet-in-Residence.
"hand ‘em another $350 billion to fight Communism?" is the latest from BAR's Poet-in-Residence. Corporate media require American identity politics which contradict African authenticity.
Corporate media require American identity politics which contradict African authenticity.


